I don’t get out much.
I haven’t been more than walking distance away from the house in a month. And that was to see the accountant and pick up our taxes. If I had known it was our last “outing” until who-knows-when, we may have chosen something else.
We do go for a walk nearly every day, down the street and around the neighborhood. We’ve lived in the same house nearly 27 years, and yet it’s surprising what you notice in your own neighborhood when you’re not driving by. There are some hills up and down the street that we walk for cardio. Wouldn’t it be ironic if I came out of all this in better health?
Cheryl has gone grocery shopping once in this past month, with gloves and mask. Her daughter Sara delivers a few things if we run out. Otherwise, no one comes in. As Benjamin King said, there’s nowhere to go but out, and nowhere to come but back. So we stay home. This suits me, to be honest. I’m an introvert.
But today, I am venturing out. This isn’t a long drive; just three exits north on I-5. The University of California San Diego Moores Cancer Center. I have been in contact with my doctor several times. Should I keep this appointment? Yes, probably. A few days later, do you still think I should keep this appointment? Yes, the benefits outweigh the risks.

I am struck that there is no traffic. 8:30 in the morning on a Wednesday and freeway is 75 miles an hour in both directions.
I have been coming here a long time. This time, I am a bit worried about it. Scared even. The only other time I was scared to be here was January 2008, my first chemotherapy appointment. I survived that. Thrived even. I’ll survive this one. I think.
Moores is not physically connected to the hospitals. It even has its own parking structure. Even so, this time, no one could just walk in.

I was met outside the door, told to stand on the “x” and asked the screening questions. No travel, no fever, no cough, no contact with anyone who might have COVID-19. Just cancer. OK, go on in.
I make it a point to wear bright colors and try to be cheerful when I come here. Cheerful is not my natural state. I’m determined to project the image of a healthy guy while I’m here. A lot of these people are really sick. We’ve all got the Big C. The one that isn’t in the news these days.
The waiting room isn’t as busy as usual. It’s common to see couples here, or family members or caregivers. But not today. Only patients are allowed in. Every other chair is marked off so there’s anti-social distance between us all. That suits me too.
I’m here for my intravenous immunoglobulin infusion. Not a big deal. Every fourth Wednesday at 9 a.m. Without fail. When I was working, I came Saturday mornings. Now I’m retired and it’s Wednesday mornings. It’s not a coincidence that our cleaning lady comes every other Wednesday morning. She’s not coming to the house these days, but, still, here I am.
I started these eight years ago. Every four weeks. Never missed one. 13 times a year, 104 appointments, and counting. There’s no end in sight.
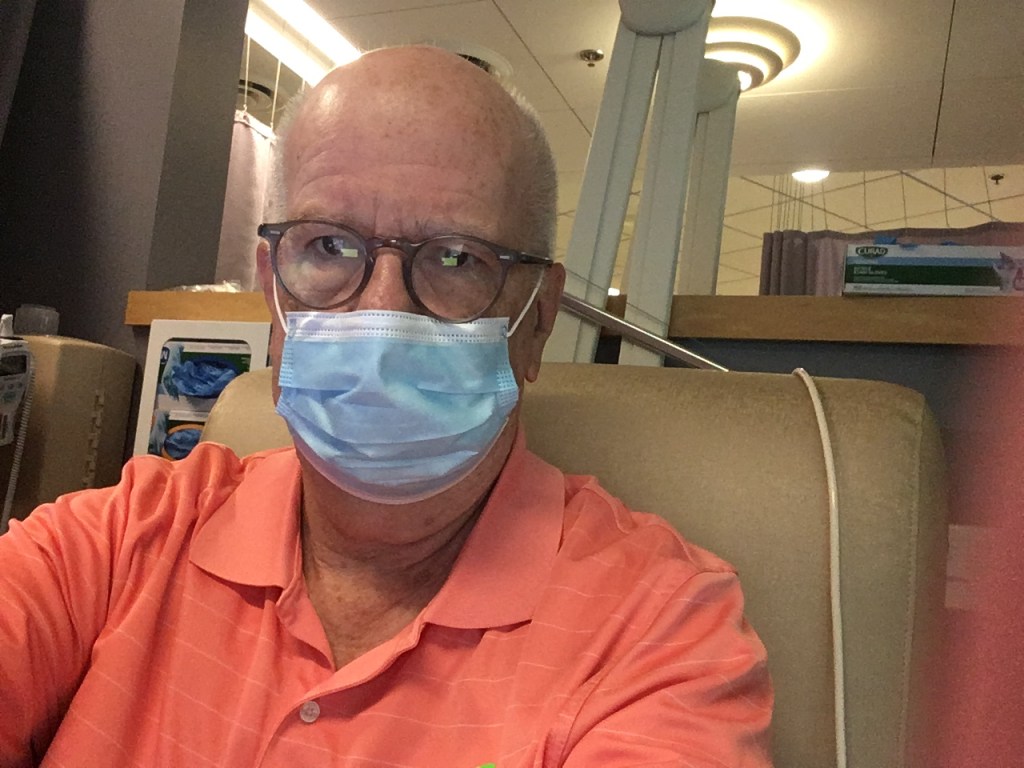
But this appointment is different. Everyone is wearing a mask. Everyone. The chair is wiped down and disinfected before I sit down. There are precautions everywhere you look.
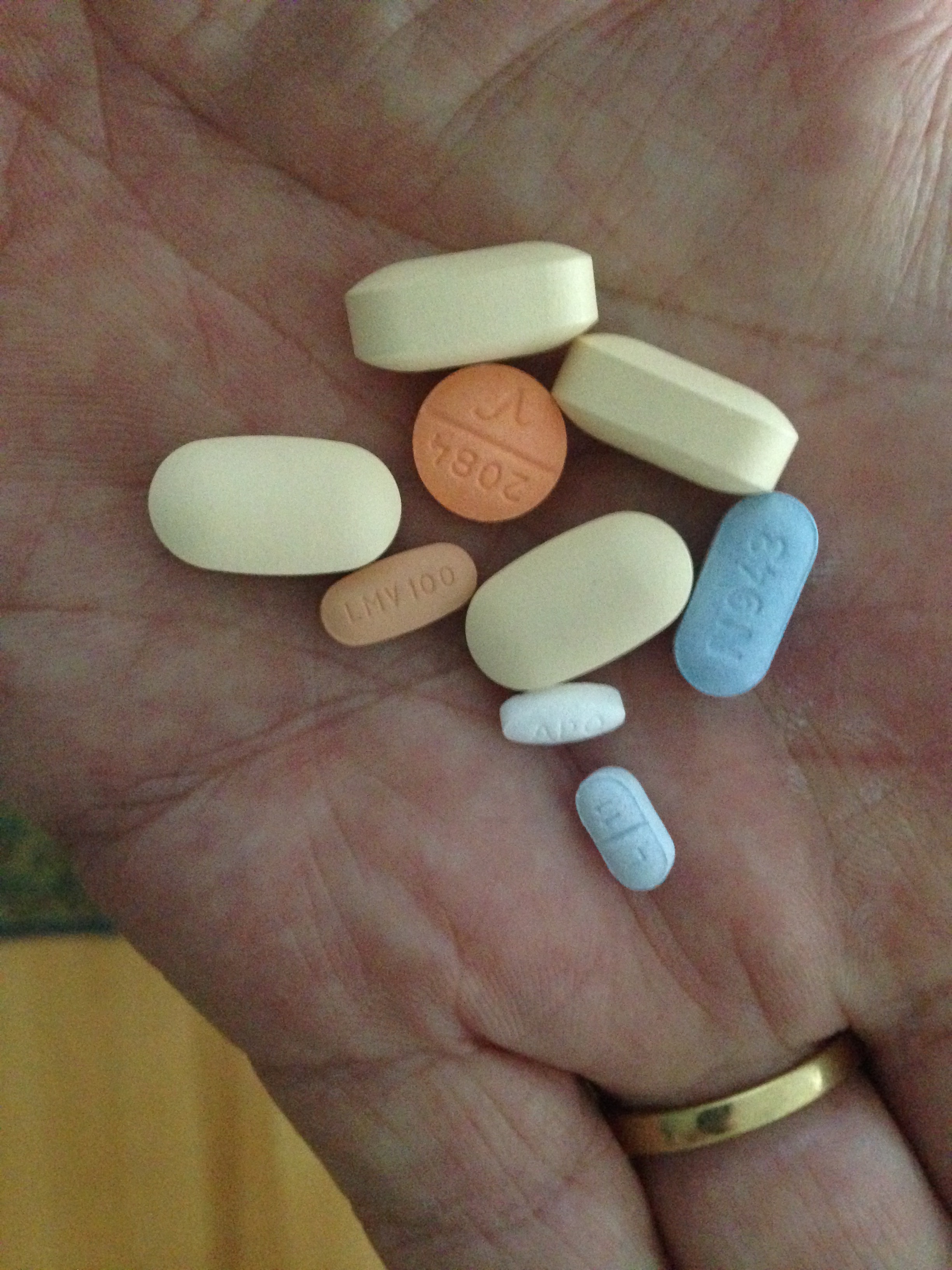
Here’s the deal. My immune system sucks. Part of that is just a fact of life with chronic lymphocytic leukemia.* Part of it is the chemotherapy that I was afraid of back in 2008 raised hell with my bone marrow and even when they can’t find leukemia cells in my blood, my marrow isn’t doing its job.
Intravenous immunoglobulin (IVIG) is immunities drawn from the plasma of about a thousand blood donors. It’s intended to boost my immune system, protect me from things like pneumonia and the flu and even just a cold. And then along comes COVID-19. IVIG won’t do squat to fight that off because blood donors don’t have COVID-19 immunities to donate. Even so, this should help with other respiratory problems and a variety of diseases, should I need it. So, hook me up.

It used to be in a bag, like most IV infusions. Nowadays, it’s a glass bottle. Looks a little like something left over from an episode of M*A*S*H.
I’ve seen the bill; these infusions cost somewhere around ten thousand dollars, each. (Don’t drop the bottle). I don’t pay anything. Let’s hear it for insurance. Let’s get it for everyone.
I’m a pro at this. I joke with the nurses that I’ve been doing this long enough they could go on a break and I would do it myself. But I’d need a third arm, at least. And, that uncanny ability to rub my arm and find a vein. I can, however, point out where to look for the best veins.
I sit down and the nurse gets started. “Ready? Little poke.” She draws a few vials of blood, starts the pump and I get out my laptop, read, do some crosswords, and, well, write this. It’s quieter here than normal. I guess that’s because everyone is here alone. Two and a half hours later, I’m done.
I’m glad to get out, get back to the car, and go straight home.
I’ll be back in four weeks. Four weeks ago, there were none of these special precautions. Just the regular precautions and I didn’t think twice about whether I should be there. Who knows what the next four weeks will bring.
I can’t imagine.
* For any other CLL nerds who might be reading this, I was diagnosed in 2007 after a physical exam. Had FCR in 2008 and got a complete response. Was enrolled in the Murano trial in late 2014. (Murano trial was Venetoclax and Rituxan. Why they named it after a Nissan SUV, I’ve no idea.) Came out of the trial MRD-Negative. It’s been just over three years with no treatment. It’s starting to show up again. My ALC is 5.5. I get IVIG because my IGA and IGM are both less than 5.